Facial reconstructive surgery includes several techniques that are associated with group of diseases mentioned on several occasions including congenital and acquired facial pathologies.
In the first group there exist many alterations such as Parry-Romberg syndrome (progressive hemifacial atrophy), Moebius syndrome (complex congenital anomaly characterized by a lack of facial expression), Binder syndrome etc. In the second group, most common causes of facial paralysis include tumors, traumatic sequels and those derived from previous medical treatments (iatrogenic).
Due to the complex functional and spatial level of the face, reconstructive techniques applied in this anatomical area maybe are the most complex and sophisticated in the speciality of Reconstructive Plastic Surgery.
Tissue transplants became extremely relevant in this field. The goal is to replace facial regions affected by cancer or recovering the function as complex as the mimic muscle system, responsible for both opening and closing of the oral and ocular sphincter and facial expression.
The process of reconstruction in patients with facial paralysis is clearly individualized as the level of nerve injury, the mechanism that caused the injury and the time of evolution determine the treatment plan and outcomes.
It is possible that an acute onset facial paralysis with no apparent cause (Bell's palsy or "frigore") is resolved with medical treatment. However, established long-term facial paralysis requires reconstructive surgery including microsurgical procedures (nerve grafts, microvascular transplantation of nerves, microvascular muscle transplants) or static procedures (suspensions, golden weight, etc).
The patient must be well aware of the complexity of these procedures as well as the "timing" of required surgery and individual approach to each case depending on the type of disorder and medical and surgical response.
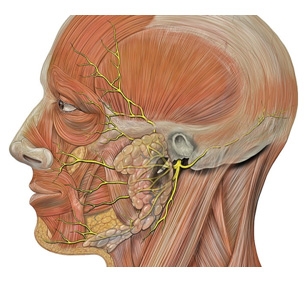
Facial paralysis means total or partial motor paralysis of the muscles of facial expression in one side of the face.
Reconstructive surgery in facial paralysis uses both static and dynamic techniques. Static techniques do not involve movement of the paralyzed side. They consist of suspensions of soft tissue hanging by the absence of muscle tone in order to obtain symmetry with the unaffected side. Dynamic techniques attempt to restore movement and lost function, requiring transplantation of tissues such as gracilis muscle flap.
When losses occur, the lining or facial deformities, sometimes associated with bone loss, almost always produces great aesthetic and functional problems. These can result from surgery to eradicate a tumor, trauma or congenital anomaly.
Plastic Surgery repairs the defect produces satisfactory results in most cases and is elective. However, there are conditions that make these techniques difficult or impossible, indicating the prosthesis for reconstruction of the defect. They are made with vulcanized silicone for flexibility, and in some cases may even be osteointegrated so as to obtain better retention and performance.
Ear reconstruction can be divided in two great categories:
Prominent ear is the most frequent pathology found in cosmetic ear surgery.
In reconstruction ear, surgery deficiencies can range from an anotia (total absence of the ear) to a microtia (a partial absence of the ear).
The timing of reconstruction is preferable between the ages of 6 to 9 years old. The intervention should be performed in the mentioned period of time, as the ears grow completely in this age and the rib cartilage, which is used as graft is totally mature and can be harvest.
Multiple techniques can be used; expanders, cartilage grafts reconstruction of the ear skeleton as well as local flaps in order to obtain the best results and symmetry.
The treatment of facial trauma begins in the acute phase. Functional and aesthetic recovery depends on good clinical diagnosis, availability of 3D-imaging and choice of appropriate surgical technique.
Based on the good knowledge of the craniofacial anatomy, pathophysiology of fractures, through clinical research in bony tissue and soft tissue reconstruction we could prevent other surgeries.
Nasal reconstruction was the first known reconstructive procedure in the history of surgery. A lot of references have been written based on in an Egyptian Papyrus since 2200 BC.
Different surgical techniques based on sensitivity and skills of the surgeon can be performed in order to recreate the structrure.
Staged reconstruction of complex defects should be the preferred technique. In small defects coverage, surgery can be performed using a local flap, although in largest defects of pedicled flaps with cartilage grafts are necessary. The cartilage provides the structure-framework, keeping the shape of the nose.
In more complex cases, we may need microsurgical techniques in order to recruit distant tissue for the coverage of the nasal mucosa, when it´s affected.


 This site complies with the HONcode standard for trustworthy health information:
This site complies with the HONcode standard for trustworthy health information: Parc Salut Mar
Passeig Marítim 25-29 Barcelona 08003
See location on Google maps
Phone: 93 248 30 00 · Fax: 93 248 32 54
Information request
© 2006 - 2024 Parc de Salut Mar · Legal notice and Privacy Police | Cookie Policy | Accessibility